
Cholesterol, Statins, and the Question We Keep Avoiding
- Healing_ Passion
- Feb 11
- 4 min read

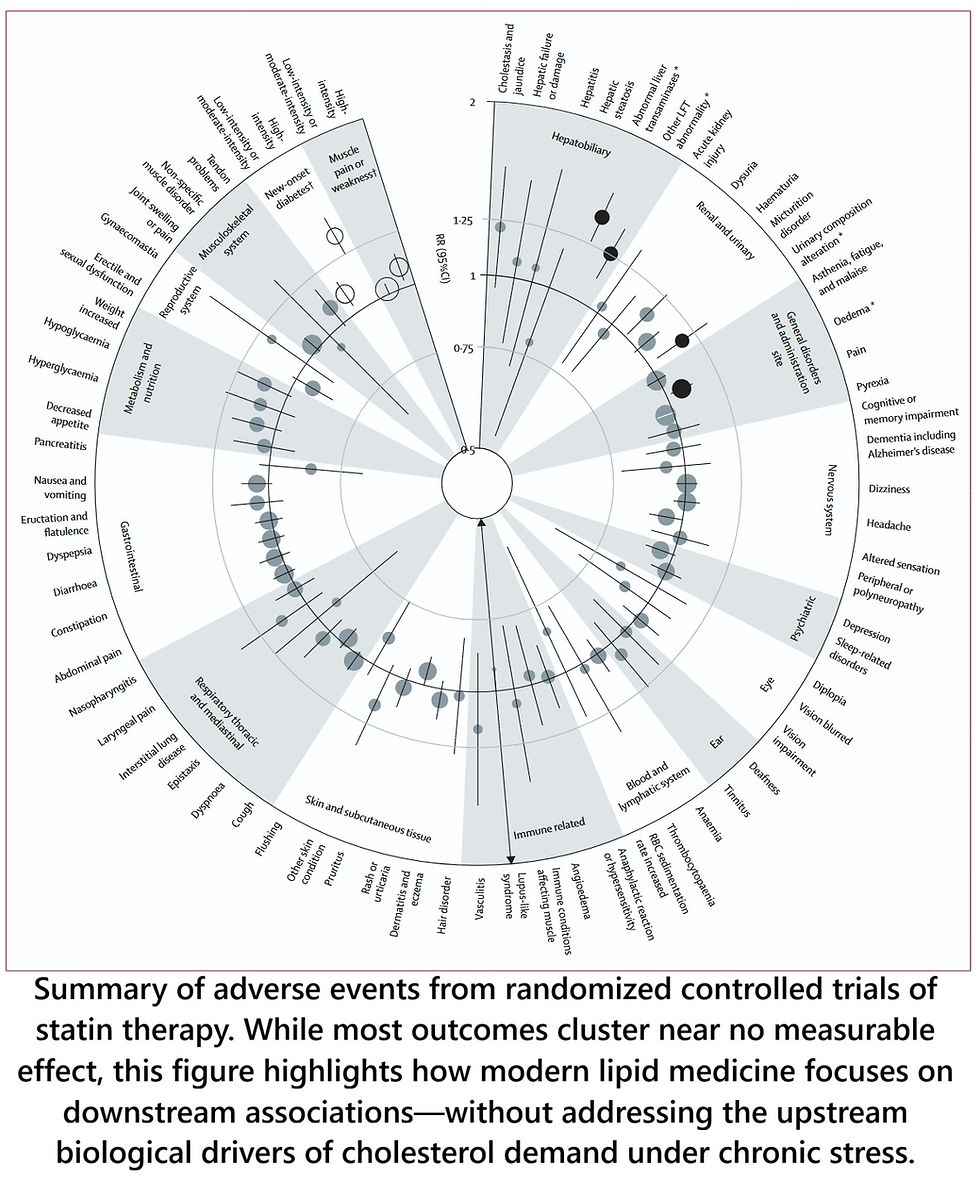
A large new meta-analysis published in The Lancet has reignited the statin debate. Headlines quickly followed: “Most statin side effects are overblown” and “Millions more people should be taking statins.”
The study itself is substantial. By pooling data from nearly 20 large, double-blind randomized trials with over 120,000 participants, the authors examined whether statins truly cause the long list of side effects commonly blamed on them.
Their conclusion was clear: for most reported symptoms—memory problems, mood changes, fatigue, kidney disease, and many others—there was no strong causal evidence in blinded trials. A few risks remained real and measurable (such as new-onset diabetes, muscle effects, and mild liver enzyme changes), but overall, statins appeared safer than public perception suggests.
That finding matters.
Fear-driven discontinuation of statins likely does harm.
But it is also where the conversation becomes dangerously incomplete.
Critics Are Right About One Thing
Several thoughtful critics have pushed back—not by rejecting the data, but by questioning the interpretation.
They point out (correctly) that:
“Not statistically significant” does not mean “biologically impossible.”
Some outcomes trend toward harm but fail to cross conventional statistical thresholds.
Randomized trials are not designed to capture every long-term, subtle, or subgroup-specific effect.
Headlines tend to flatten nuance.
These critiques deserve to be heard. But they still circle around the same downstream question:
How safe is it to suppress LDL cholesterol?
That question—important as it is—misses a more fundamental one.
The Question We Rarely Ask
Most cholesterol in your blood does not come from food.
It is produced internally, mainly by the liver, under tight regulatory control.
So the deeper question is not:
How do we lower LDL further?
It is:
Why does the body feel the need to produce and circulate so much LDL in the first place?
Until we ask that, we are managing numbers, not biology.
What Current Practice Quietly Reveals
Modern lipid management follows a familiar escalation:
Start with a statin to suppress cholesterol synthesis
Increase the dose when LDL rebounds
Add ezetimibe when the body compensates by absorbing more cholesterol from the gut
Add a PCSK9 inhibitor when LDL still remains “too high,” forcing the liver to pull LDL out of circulation
This stacking of medications is framed as progress.
Biologically, it tells a different story.
Each added drug exists because the body pushes back.
When synthesis is blocked, absorption rises.
When absorption is blocked, clearance brakes engage.
When clearance brakes are overridden, lifelong suppression becomes necessary.
That is not a passive system misbehaving.
That is homeostasis defending something essential.
Cholesterol as a Stress-Adaptation Resource
Within an ERM (Exposure-Related Malnutrition) and stress-adaptation framework, cholesterol is not just a cardiovascular risk marker. It is a strategic biological resource.
Among its many roles—membrane repair, immune signaling, neural integrity—one stands out under chronic stress:
Cortisol production
Cortisol is the hormone that keeps blood sugar available, blood pressure stable, inflammation contained, and the organism functional under threat. Failure of cortisol production is not a long-term risk—it is immediately life-limiting.
Cortisol is synthesized from cholesterol.
During chronic, unresolved stress:
Cortisol demand stays high
Shutdown and recovery never fully occur
The body prioritizes cholesterol availability
LDL production and trafficking increase to secure supply
From this perspective, LDL is not “excess.”It is a delivery system.
Why Suppression Works—but Never Resolves the Problem
Lowering LDL undeniably reduces cardiovascular events. That matters.
But LDL-centric therapy:
Reduces exposure
Buys time
Lowers risk downstream
What it does not do is resolve the signal that drove LDL production in the first place:
Chronic inflammation
Persistent stress signaling
Mitochondrial inefficiency
Impaired repair and recovery
Micronutrient and energetic constraints
That is why residual risk remains high—even at very low LDL levels.
That is why escalation never truly ends.
That is why withdrawal often leads to rebound hypercholesterolemia.
The system is still trying to meet a demand.
A Different Way to Read the Statin Debate
The new meta-analysis tells us something important:
Many feared statin side effects are not causally supported in blinded trials.
Statins are safer than many believe.
But it does not tell us why LDL is elevated to begin with.
Critics are right to warn against simplistic conclusions.
Advocates are right to value LDL lowering.
Both sides miss the upstream biology.
The Reframe That Matters
Instead of asking only:
How low should LDL be?
We should also ask:
What unresolved biological stress makes cholesterol production feel non-negotiable?
When that question enters the conversation, cholesterol stops being a villain or a virtue.
It becomes a signal.
And medicine can finally move from:
suppressing adaptationto
restoring resolution.
Bottom line
Most blood cholesterol is internally produced.
The body actively defends its availability.
Medication stacking proves demand persists.
LDL lowering reduces harm—but does not explain the cause.
Chronic stress adaptation, not dietary excess alone, drives long-term cholesterol demand.
Until we address why the body needs LDL so badly, we will keep piling up better blockers—while the original signal quietly remains.
Cholesterol Treatment Trialists’ (CTT) Collaboration. (2026). Adverse events attributed to statin therapy in randomized controlled trials: A meta-analysis of individual participant data. The Lancet, 407(10xxx), xxx–xxx. https://doi.org/10.1016/S0140-6736(25)01578-8



Comments