
When Healing Stalls: Why Energy, Not Inflammation Alone, Determines Recovery
- Healing_ Passion
- Dec 19, 2025
- 3 min read

We often think of healing as something the body does automatically. Cut the skin, fight the infection, calm the inflammation—and recovery should follow.
But what if healing doesn’t fail because the signal is wrong…What if it fails because the energy to complete the job is no longer available?
A recent study published in Cell Metabolism offers a striking demonstration of this idea—and helps explain a central concept behind Exposure-Related Malnutrition (ERM).
Healing Is an Energetic Process
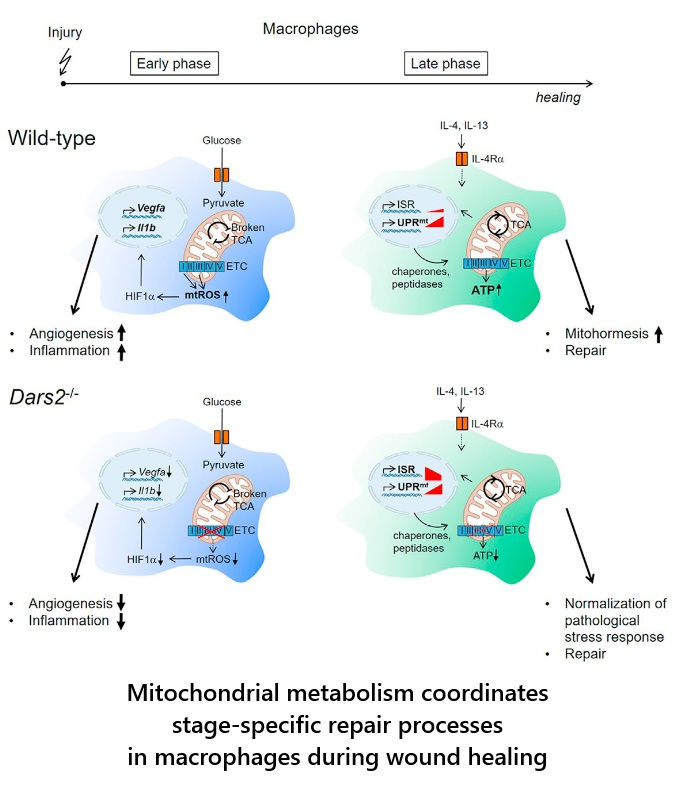
In the study, researchers examined immune cells called macrophages, which play a critical role in tissue repair. These cells must shift through phases:
Contain damage
Clear debris
Rebuild tissue
Stand down
Each phase requires a different metabolic state. Early responses rely on rapid, defensive energy use. Repair, however, requires mitochondrial capacity, protein synthesis, and anabolic completion.
When the researchers disrupted mitochondrial protein synthesis—even without fully shutting down energy production—macrophages could no longer complete this transition. The result was not excessive inflammation, but stalled healing.
The cells were activated.
The signals were present.
But recovery failed.
This Is ERM at the Cellular Level
ERM describes a state where the body adapts to chronic exposure—stress, inflammation, infection, toxins, under-nutrition—by reallocating limited energy toward survival and defense.
Short-term, this is adaptive.
Long-term, it becomes costly.
In ERM, the problem is not that the body stops responding.
It is that recovery becomes energetically unaffordable.
This study shows exactly that:
Immune cells entered a stress-adapted holding pattern
Mitochondrial stress activated protective pathways
But cells could not re-enter the anabolic phase required for tissue repair
This is not a collapse.
It is prolonged containment without resolution.
Why Signals Alone Are Not Enough
Even when the researchers provided strong reparative signals (IL-4 and IL-13), the cells could not fully recover if mitochondrial capacity was compromised.
This matters clinically.
It suggests that in chronic conditions—autoimmune disease, persistent fatigue, slow wound healing, post-infection syndromes—the issue may not be “too much inflammation,” but insufficient energetic capacity to finish healing.
In ERM terms:
The system receives the instruction to rebuild, but the metabolic budget is already spent.
From Wounds to Whole-Body Health
While this study focused on immune cells in tissue repair, the principle extends far beyond wounds.
The same energetic logic applies to:
Muscle regeneration
Gut barrier repair
Neuroimmune recovery
Hormonal resilience
Stress adaptation and aging
Across systems, repair is the most energy-demanding phase. When energy is chronically diverted toward defense and maintenance, regeneration becomes optional—and eventually inaccessible.
This is why ERM emphasizes:
Not just nutrient intake, but bioenergetic availability
Not just stress exposure, but recovery capacity
Not just activation, but resolution
You’re Not Broken—You’re Exhausted
One of the most important messages from both this study and the ERM framework is this:
Failure to heal does not necessarily mean irreversible damage.It often reflects unresolved energetic debt.
When the body cannot afford recovery, it adapts by staying in survival mode.
Recognizing this shifts the clinical question from:
“What is wrong?”
to:
“What has made recovery unaffordable—and how can we restore it?”
That reframing opens the door to earlier recognition, gentler intervention, and more realistic paths back to resilience.
Willenborg, S., Sanin, D. E., Jais, A., Ding, X., Ulas, T., Nüchel, J., Popović, M., MacVicar, T., Langer, T., Schultze, J. L., Gerbaulet, A., Roers, A., Pearce, E. J., Brüning, J. C., Trifunovic, A., & Eming, S. A. (2021). Mitochondrial metabolism coordinates stage-specific repair processes in macrophages during wound healing. Cell metabolism, 33(12), 2398–2414.e9. https://doi.org/10.1016/j.cmet.2021.10.004



Comments